
Colestzen Reviews 2026 Does It Live Up To The Hype — Genuine Buyer Guide

Explore Colestzen reviews in 2026, featuring genuine buyer feedback and user experiences. Discover how this product fares in the cardiovascular health niche.
Explore Colestzen reviews in 2026, featuring genuine buyer feedback and user experiences. Discover how this product fares in the cardiovascular health niche.
Read GlycoMute reviews 2026 with verified buyer stories, before‑after photos, and honest user feedback that show real blood sugar support experiences today.

Curious if FemiCore lives up to the hype in 2026? We break down the science and real‑world results to answer does FemiCore really work for bladder health.
Explore authentic 2026 FemiCore reviews: real buyer stories, before‑after photos, verified feedback, and honest experiences that showcase true bladder‑support r

Read authentic Neuro Energizer reviews for 2026, featuring verified buyer feedback and real user experiences that reveal if the supplement lives up to the hype.

Explore authentic Visium Plus reviews for 2026, featuring verified buyer stories and real user feedback to help you decide if this eye‑support supplement works.
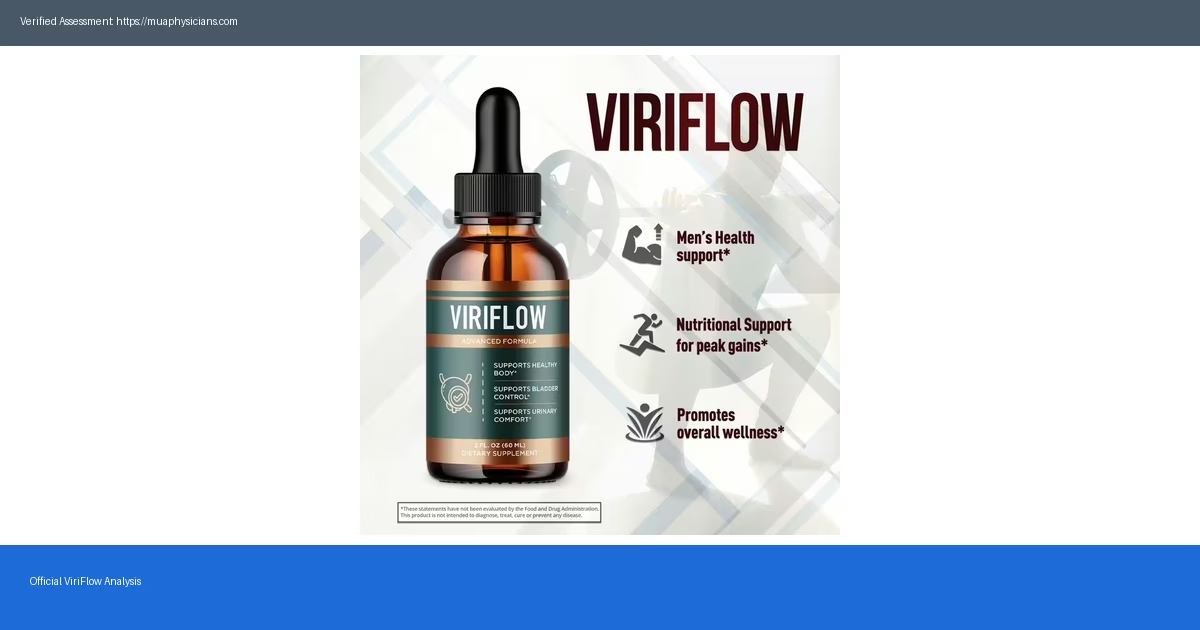
Read ViriFlow reviews 2026: real customer stories, verified feedback, and before‑after results that show genuine experiences with this prostate support.
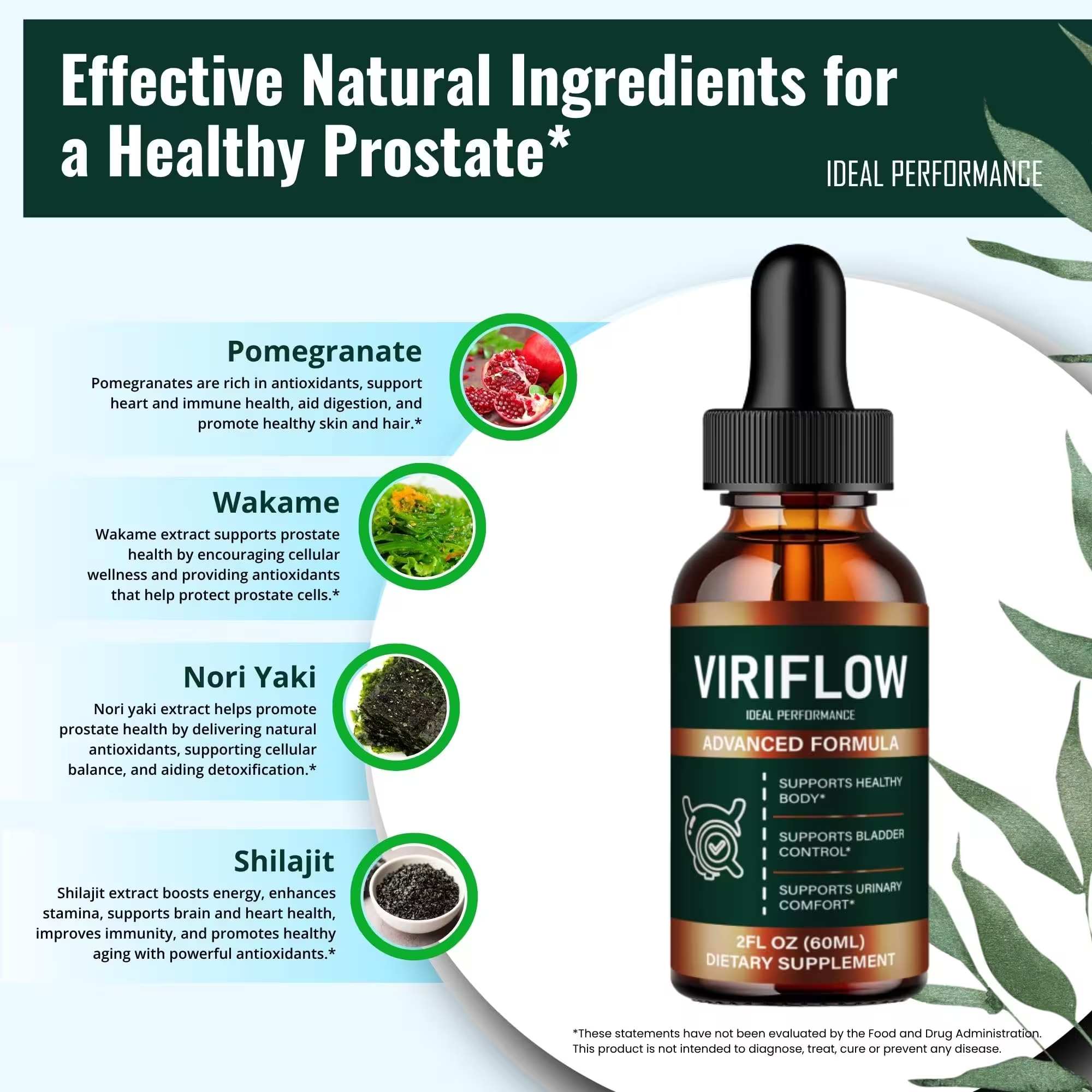
Dive into ViriFlow reviews for 2026, discovering real user experiences and verified buyer insights on prostate health without claims of treatment or cure.

Read unbiased TerraCalm reviews 2026: real buyer stories, verified feedback and what users actually say about this nail care solution. Plus pros and cons.

This article focuses on real customer reviews, verified buyer feedback, and honest user experiences with EyeFortin. Read our full 2026 breakdown of EyeFortin be